Technology in everyday life
Guidance
During the development or use of technological devices, the individual needs of the person with cognitive impairments (e.g. dementia or MCI) and carer should be considered. This includes not only everyday technology, but also surveillance technology (ST) and technology used during cognitive training sessions. Increased awareness and offered assistance is recommended.
Explanation and Examples
People with dementia tend to face more and other difficulties than people with MCI when using relevant everyday technologies such as cash machines, calling or texting with a cell phone or using a DVD player, and thus need more assistance in technology use. This may also be the case with ST and technology used for cognitive training.
For example, ST are often presented as a neutral technology, which enables carers to minimise risk. However, the views of users have not been sought by ST developers, which limits the usefulness of ST and suggests the need for the empowerment of user groups. Therefore, a study of audience reception was undertaken through focus groups, online discussions (Netherlands) and PPI (UK). Hereby people with dementia could speak for themselves, which has allowed their needs to be compared with carers. There was no clear recognition that such needs differed between people with dementia and carers, and it has not previously been recognized that this leads to a mismatch between a user’s situation and the product design and how this plays out in the acceptance and use of ST. Although, carers and people with dementia have not yet reached an agreement on the privacy debate and on how the media should portray dementia, it is clear that carers often tamper with ST to make up for a lack in current designs. The results suggest that ST are being resold or rebranded by providers to use for dementia, whilst users may experience physical and cognitive barriers to using such technologies for safety reasons.
Regarding technology for cognitive training: As older people have little experience with technological devices, and so may experience problems, professionals involved in cognitive training should monitor training sessions from the outset. The professional must observe and ensure the ability of the older person to understand the instructions given through the technological device, so that the person can really benefit from the cognitive training by computer. For example, in sessions with GRADIOR, a cognitive rehabilitation program, there is always a professional in charge who helps older people to understand the exercises they may experience difficulty with.
Read more >
Guidance
When selecting technologies for use in public spaces, procurers should involve occupational therapists and designers with expertise in dementia, and people living with dementia. Public space technologies should:
- have the most cognitively enabling and inclusive design features (i.e. minimal steps and memory demands),
- be sited in the most supportive physical location (i.e. secure vestibule, busy thoroughfare) and
- identify and account for wider sociocultural preferences (i.e. continued face-to-face services).
Explanation and Examples
Life outside home in most countries increasingly demands the use of everyday technologies (ETs i.e. transport ticket and parking machines, ATMs, airline self-check in machines, fuel pumps). However, ETs can present challenges, particularly for people with dementia, and differences in design and location may mean some ETs are easier to use than others.
To investigate variation in the challenge of ETs; the Everyday Technology Use Questionnaire was administered with 315 people with and without dementia (73 in Sweden, 114 in the USA, 128 in England) in a cross-sectional, quantitative study. Modern statistical analysis found 5/16 public space ETs differed in challenge level between countries (specifically: ATM, airline self-check-in, bag drop, automatic ticket gates, fuel pump).
These differences result from variation in design features or siting of technologies. However, they may also be due to differing habits between users in different countries (i.e. necessity and frequency of use, preference for particular modes of transport, concerns about security, embarrassment) or varying progress towards technologised rather than face-to-face services (i.e. towards cashlessness).
Taking account of inter-country differences could lead to selecting the most useable technologies and services. This could improve inclusiveness of public space internationally for older adults with and without dementia.
Read more >
Guidance
People with dementia reporting new difficulties using everyday technologies should be offered a comprehensive assessment by an occupational therapist. While everyday technology can be assistive to everyday activities, in some cases, a pattern of detechnologising indicates instability in the person’s wider pattern of participation and may indicate a need for support, or change in housing situation.
Explanation and Examples
Everyday life, including outside home, more and more involves the use of everyday technologies (mobiles, smartphones, ATMs, transport ticket machines etc), which could even influence the places that people go to. A cross-sectional, quantitative study with 128 older adults with and without dementia in England was conducted using the Everyday Technology Use Questionnaire and the Participation in Places and Activities Outside Home questionnaire.
Results of statistical analyses confirmed that for some people; going to a lower amount of places was related to perceiving a lower amount of technologies relevant in daily life and living in a relatively more deprived area. A subsequent case study was conducted with 13 rurally dwelling older adults from the same sample (using the same questionnaires with additional interview notes, observations, maps, subsequent relevant document collation i.e. mobile and internet network availability reports).
Findings highlighted a person could perceive detechnologising, particularly around the home and garden, as one of several signs of vulnerability when living alone rurally. Such vulnerability was then a sign of a need for support to make living at home more tenable, including to increase safety in the grounds surrounding home, or was a sign of a need to relocate.
Read more >
Technology for meaningful activities
Guidance
Consider using smartphone-based experience sampling apps to measure everyday fluctuations of variables such as mood, behaviors, or cognition in people with mild cognitive impairments or carers of people with dementia to better understand variations in daily experiences.
Explanation and examples
The ‘Partner in Sight’ intervention for carers of people with dementia, the ‘Monitor-Mi’ study (feasibility of the experience sampling method (ESM) in people with MCI), and the development of two cognitive tasks (mDSST; mVSWMT), all included the experience sampling method (ESM). These studies are first steps towards a better understanding of and support for people with cognitive impairments, such as MCI or dementia, and their carers in everyday life.
The results indicate positive effects on carers’ well-being, feasibility of using the ESM in people with MCI, and internal validity when assessing momentary cognition in healthy older individuals. The experience sampling method has a high ecological validity with a reduced memory bias, allows to see fluctuations, and uncovers a complex picture of affect, behaviour, and other variables in everyday life. It can be used to increase awareness of own daily patterns and motivate behavioural changes towards more meaningful activities.
Read more >
Guidance
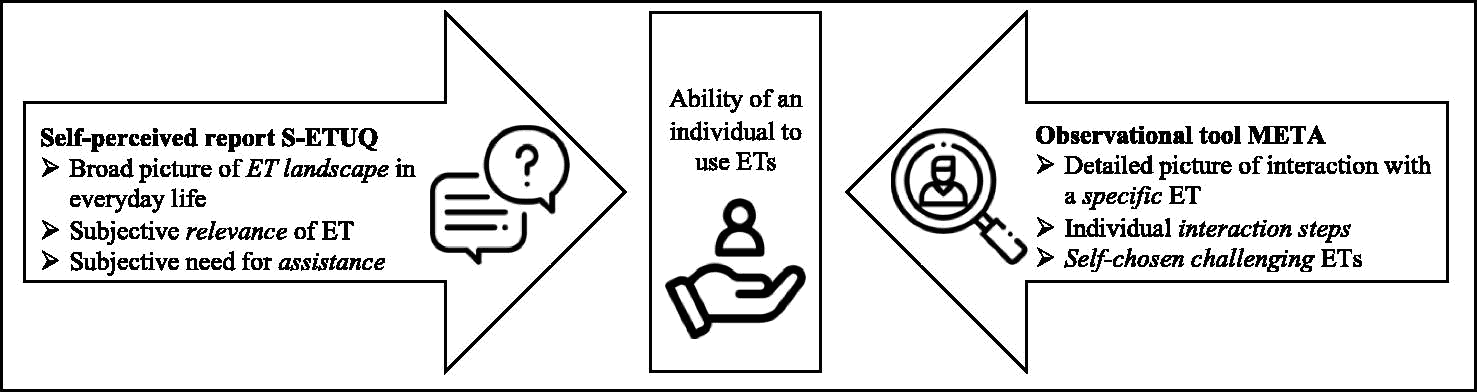
To understand the ability of the elderly with cognitive impairments to use everyday technology observe the interaction but also ask about their views.
Explanation and examples
Via an observation (guided by the META), the person-technology interaction can be described in detail, e.g. does the person press buttons/the screen with an adequate force or are steps performed in a logical order. This can help to determine which elements of a specific technology are causing problems and might be particularly useful for designing intervention and the development of technology. Through a self-perceived report (S-ETUQ), the individual can reflect on a wider range of technologies and the impact of technology use to perform well in (in relation to) everyday life can be depicted. For example, if someone has problems using the ticket machine for public transport or the ATM, this might impact participating in society; if the individual has problems with using the dishwasher or vacuum cleaner, this might impact the hygiene and well-being at home.
Read more >
Health care technologies
Guidance
Nursing homes providing care for people with dementia should consider introducing portable devices in addition to desktop devices for electronic patient records (EPR). Devices should not disrupt or invade residents’ privacy.
Explanation and Examples
Portable devices have been shown to increase efficiency in some instances as they allow staff to record data into the EPR at the point of care instead of at the end of the shift. This enables staff to spend more time providing care to residents, particularly for residents with dementia and complex needs. Portable devices can support person-centred care by allowing immediate access to care plans with vital information about residents, such as dementia diagnosis. Rapid access to care plans is important for staff retrieving information about individuals who are at the nursing home temporarily on respite; for those residents who may be unable to recall personal information; and for those staff who work infrequently in the home and are unfamiliar with residents. However, it should be taken into consideration that some staff may prefer desktop devices based on ease of use when completing substantial documents. During the development of portable devices for nursing homes, the impact that such devices could have on residents should be taken into account and staff should explain the purpose of EPR devices to residents and family members who may be unfamiliar with the technology.
Read more >
Guidance
Applications that should be incorporated into EPR systems used in nursing homes providing care for people with dementia include a spell-check, a copy and paste function and a keyword search function. Log-in processes should be rapid and secure.
Explanation and Examples
The presence of a spell-check has been described as saving time on proofreading, as well as increasing legibility and comprehension of documentation. This allows for more time to be spent with residents with dementia in direct care, and for correct care to be provided. A copy and paste function also saves time by allowing staff to easily transfer information across sections of the EPR where information is often required to be replicated. A keyword function allows staff to enter a keyword and jump to the relevant section in a resident’s notes, allowing for more efficient retrieval of information, important in situations when a resident is unable to recall personal information. Rapid log-in processes should reduce barriers to using the EPR, as slow log-in processes have been found to prevent staff from accessing information about residents before delivering care, and have meant staff have been forced to pass on information about residents verbally instead of entering it into the EPR. This may mean important information regarding any sudden changes in an individual’s condition might be missed.
Read more >
Guidance
Developers of EPR systems for dementia care should consider including a function allowing for the automated generation of graphs to show trends in data, and an accompanying function to prompt staff about changes in a resident’s condition. In addition, functions allowing for the automated generation of care plans from assessment data, and alerts to prompt staff to create or update a new document in the EPR may be of value to nursing homes. Interoperability should be a goal for the future.
Explanation and Examples
Automatic generation of graphs displaying trends in a resident’s condition increases visibility of changes, allowing staff to more rapidly identify and respond to changing care needs. For example, graphs showing changes in weight, which can commonly affect individuals with dementia. Furthermore, through the incorporation of artificial intelligence (AI), some EPR systems are able to analyse resident data and provide alerts to staff about potential risk factors. For instance, alerts to warn staff about potential skin breakdown, important for those residents with dementia receiving end-of-life care, who may be spending considerable amounts of time in bed and have reduced fluid intake. Automatic generation of care plans from assessment data could save staff time in administration, as well as automatic alerts incorporated into the EPR that prompt staff to update care plans, meaning optimal care can be planned and provided to individuals with dementia. Finally, EPR systems should be interoperable, so that staff can access and communicate relevant information securely over the internet with external healthcare providers, instead of using paper records.
Read more >
Guidance
EPR systems should include the necessary assessment templates for use in the care of people with dementia, as well as space for entry of free text and to upload photos of residents. Electronic assessment forms and care plans for dementia care should use formalised nursing language to prompt the entry of correct information, and structured templates that guide staff through body systems, leading to comprehensive care plans.
Explanation and Examples
EPR systems in nursing homes have been found to omit the appropriate scales and assessments required by nursing staff caring for people with dementia. For instance, staff stated that they require the MMSE assessment, the QUALID scale, and the Barthel Index of Activities of Daily Living incorporated into the EPR. Furthermore, staff have identified incorrect nursing language in electronic forms, meaning important information is not recorded. For example, the omission of the term ‘dementia diagnosis’ from assessment forms meant that nurses were not entering this information about residents. By including the appropriate structured forms for data entry with formalised nursing language, Artificial Intelligence (AI) tools can be more successfully integrated into the EPR. Space for photos of residents is important for new staff when learning residents names and for confirming identities of residents when required, and structured body templates included into the EPR have been identified as a useful visual prompt for completing assessments. Staff also require space to enter life stories, and space for free data entry for additional notes and observations. For example, changes in the behaviour of a resident with dementia.
Read more >
Guidance
Electronic assessment forms and care plans used for planning dementia care in nursing homes should prompt staff to consider the following needs of residents: activities, maintaining previous roles, reminiscence, freedom and choice, appropriate environment, meaningful relationships, support with grief and loss, and end-of-life care.
Explanation and Examples
The themes above have been described by people with dementia in various studies exploring their self-reported needs and experiences in nursing homes. Developers should therefore consider including these themes into electronic assessment and care plan templates as prompts for nursing home staff to explore with residents.
Read more >
Social Health Domain 1: Fulfill ones potential and obligations
Guidance
People with Young Onset Dementia can experience difficulties using technology or particular platforms for online peer support. Facilitators of video meetings and moderators of text-based platforms (such as Facebook groups or discussion forums) should provide clear guidance on how to use the platform and be available to offer technological assistance where needed.
Explanation and Examples
Our study, including 20 people with Young Onset Dementia across 4 focus groups, showed that most of them experienced difficulties with the online meetings at some point. This included having difficulties getting into the Zoom meeting and installing or updating the software on their devices. Some more specific recommendations included:
- The facilitator of video meetings should send out timely reminders, preferably also on the day of the meeting, including the link to the meeting. This reduces the risk that someone cannot find the link.
- The facilitator should provide a clear step-by-step guide on how to install and use the necessary software.
- The facilitator should open the meeting 10-15 minutes beforehand to allow people to get in and if needed provide remote support (e.g. via email, WhatsApp, or a phone call).
Read more >
Guidance
It is important that the online peer support group is a safe and non-judgemental environment for everyone in the group. Most of all it is a platform for members to express themselves and support one another. It is the role of the facilitator to make everyone feel included, heard, and safe.
Explanation and Examples
Through 4 focus groups including a total of 20 people with Young Onset Dementia, and 9 individual interviews with people with Young Onset Dementia, people highlighted the importance of the role of the facilitator. Additionally, through speaking with online group facilitators, they shared what they think is important and what helps them to run a meeting well. Facilitators should:
-
Have good listening skills and not take over the conversation too much, but let the group decide what to discuss and what is important.
-
Make every member of the group feel included and give everyone a chance to speak. If people raise their hand, make sure to address everyone in order.
-
Make sure not one person dominates the conversation.
-
Call out bullying or abusive behaviour or language.
-
Check in with someone after the meeting if they appeared distressed or upset, or if they left suddenly without explaining why.
-
Really get to know the members, for example by meeting with them one-on-one before they join the group. In this way facilitators can learn what someone is expecting from the group, and what their needs are.
Read more >
Guidance
Dementia associations’ websites are an ideal place to provide advance care planning information to a wide public. If information about advance care planning is provided, dementia associations should ensure balanced content. Websites should address not only legal and medical information, but also practical guidance on how to engage in and communicate about advance care planning.
Explanation/examples:
Advance care planning is a process that enables individuals to define goals and preferences for their future care. As people with dementia have a high risk of cognitive decline, advance care planning is important. Many people use the internet to find health information. Some of the most consulted sources to search for specific information about dementia are the websites of dementia associations. We conducted a content analysis of dementia associations’ websites in Europe regarding advance care planning information. We included 26 dementia associations’ websites from 20 countries and one European association, covering 12 languages. Ten websites did not mention advance care planning. The information on the remaining 16 varied in terms of themes addressed and amount of information. Legal and medical themes were prominent, while other key advance care planning themes such as communication with family, communication with health professionals, sharing of decisions and the identification of personal values and life goals seem largely to be under-addressed. This is an important gap, given that the drafting of advance directives should be preceded by a process of communication between the person with dementia, their family and their healthcare providers.
Read more >
Social Health Domain 2: Manage ones own life and promote independence
Guidance
See recommendation no. 3.1.4.1
Read more >
Guidance
See recommendation no. 3.1.4.2
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
See recommendation no. 3.1.4.1
Read more >
Guidance
See recommendation no. 3.1.4.2
Read more >
Guidance
The design of some existing pet robots for people with dementia do not sufficiently consider their preferences. For example, while some pet robots are designed to resemble unfamiliar animals such as a dinosaur or seal, people with dementia seem to prefer more familiarly designed pets, such as domestic animals like cats and dogs. As little research has been done into pet robot design preferences of people with dementia further investigation is needed.
Explanation and Examples
One of the most researched and used pet robots in dementia care is PARO, a robotic baby harp seal. The developer of PARO anticipated that users are likely to be more accepting of PARO, since they are less likely to have experiences and expectations of a seal. However, Bradwell and colleagues found that older adults including people with dementia have expressed a preference for familiar animals such as cats and dogs. A qualitative study uncovered similar findings – Care providers in nursing homes expressed that residents with dementia may prefer and react better to familiar animals. In line with a person-centred approach to care, the use of pet robots should account for the preferences and needs of people with dementia. However, there is a lack of studies that have explicitly investigated such design preferences. More studies are necessary to bridge this gap.
Read more >
Guidance
People designing psychosocial interventions for people with dementia should be aware that viewing generic, rather than personal photographs, can also be a meaningful activity for the person with dementia. Moreover, viewing these photos digitally was found to be either similar to or better than viewing conventional printed photos.
Explanation and Examples
There is evidence that using generic photos, versus personal family photos, in psychosocial interventions for people living with dementia can be more effective in promoting social interaction and eliciting stories with emotional and personal significance. Generic photos may feel less threatening compared to using personal photos in conversation with the person with dementia, the conversation that arises becomes more flexible and less demanding of remembering specific people or events. This can lead to better social interaction, mood, and eventually, better quality of life for the person with dementia.
Generic photographs can be more accessible and easier to acquire, lessening the time needed to, for example, ask for and collect family photographs from relatives (if these are still available). It has the potential to be cost-effective as well (compared to other art-based activities like museum visits), and has the potential to transcend societal or cultural differences.
These benefits may be even more pronounced, when generic photos are used in a digitalized format, as previous research showed that viewing digitalized photos is similar to or better (due to the pleasurable experience of using virtual reality technology; Tominari et al., 2021; Xu & Wang et al., 2020) than viewing conventional printed photos.
Read more >
Guidance
The choice for a tablet-based intervention should be based on an assessment of the characteristics of the tablet-users and their specific needs and potential to benefit from the intervention. Care providers should consider prioritizing people with MCI and younger people with MCI/mild dementia to receive tablet-based interventions.
Explanation and Examples:
Evidence from the FindMyApps project showed that on average, tablet interventions could be effective to promote participation in social and other meaningful activities. However, the results also showed that tablets seem to be particularly effective for people with a diagnosis of MCI compared to those with a diagnosis of mild dementia. Regardless of the diagnosis, the results also suggest that younger people with MCI/mild dementia also benefit more from tablet-based interventions than older people. The choice for a tablet-based intervention should therefore be based on an assessment of the tablet-user characteristics, in addition to their needs and potential to benefit from it.
Read more >
Technology for meaningful activities
Guidance
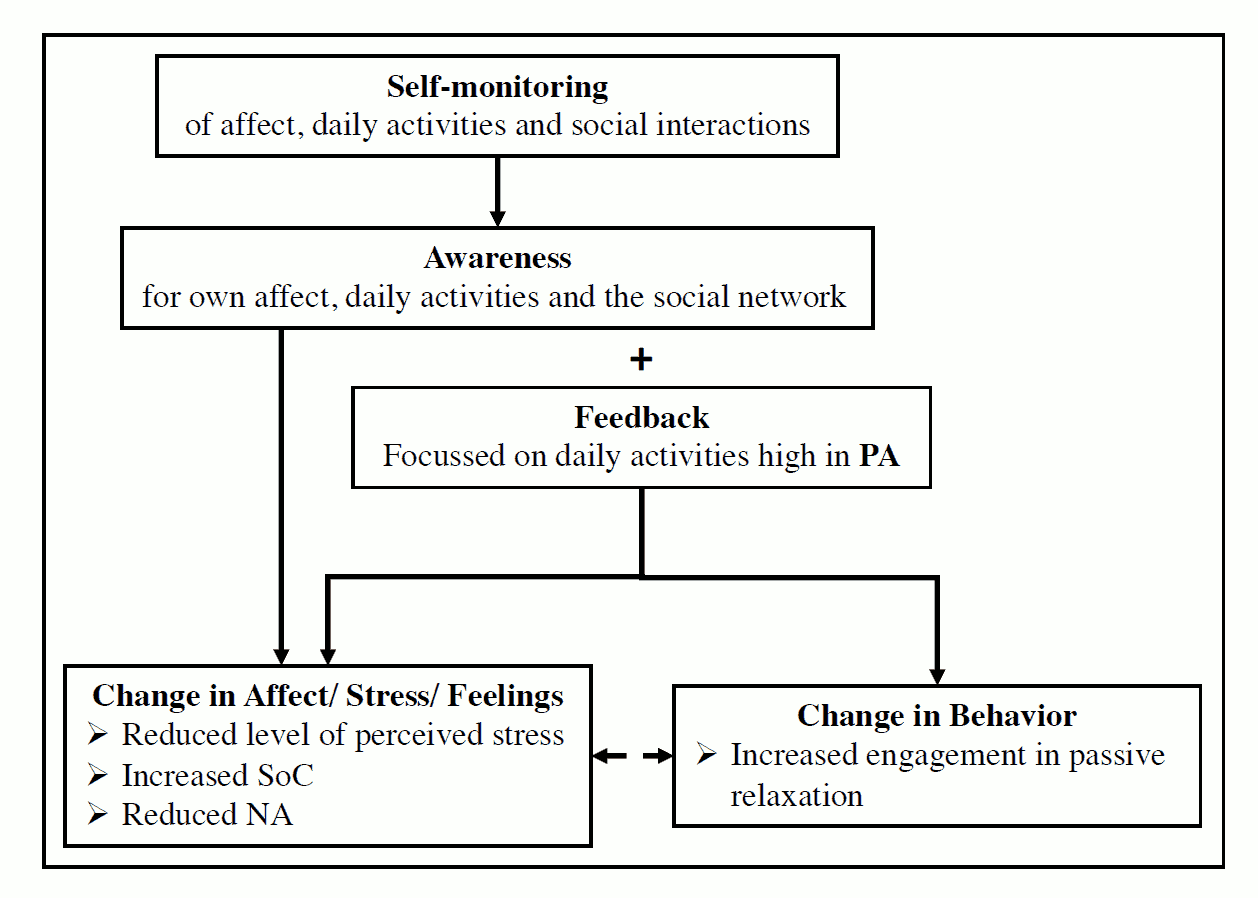
When using smartphone-based digital self-monitoring/experience sampling in carers of people with dementia, consider providing personalized feedback to promote emotional well-being and stimulate the undertaking of more activities they enjoy (e.g. relaxation activities).
Explanation and examples
‘Experience sampling’ (ESM)-based smartphone apps can offer solutions to raise awareness of enjoyable activities, strengthen learned coping strategies, and provide (long- term) support in everyday life. The ‘Partner in Sight’ intervention has been found to decrease perceived stress as well as negative affect, and to increase sense of competence in carers.
However, an increase in passive relaxation activities was only achieved with personalized feedback. Long-term support could be achieved by adding additional features, such as booster sessions, micro interventions (short version of the original intervention) or ad-hoc counseling after the main intervention period, through cost-effective and common technologies (smartphone apps, webpages, emails, telephones).
Read more >
Guidance
People with dementia can have difficulty finding apps for self-management, meaningful activities and social participation that match their needs, interests and abilities. A tool that helps them find such apps is therefore recommended.
Explanation and example
People with dementia often experience unmet needs in their self-management, meaningful activities and social participation. Apps and technological interventions can potentially help them fulfil these needs and also decrease the burden for caregivers.
The last decade many apps have been developed that can support people with dementia in managing daily life, engaging in activities and staying in touch with their social network. However, people with dementia may have difficulty finding apps that match their needs, interests and abilities, FindMyApps is a selection tool that aims to help people find, download and use apps for self-management and meaningful activities, which are dementia-friendly and meet their needs, interests and capabilities.
A randomized controlled exploratory trial into the effectiveness of FindMyApps showed that people with dementia who were offered this tool more frequently downloaded and used apps for self-management and meaningful activities than people who did not have access to this tool. This confirmed the usefulness of the tool. Therefore, a tool such as FindMyApps is recommended for people with dementia and their caregivers to ease the search for suitable apps.
Read more >
Guidance
Meaningful activities for people with dementia have proven value for their social health. Exergaming is an innovative way of exercising in a gaming environment. This movement activity may be experienced as meaningful by the persons with dementia, is considered fun to do and has benefits for them as well as for their relatives.
Explanation and example
Exergaming was compared to usual activities in a cluster Randomized Controlled Trial among day care centres for people with dementia. In this study exergaming consisted of interactive cycling using a stationary bicycle (i.e. home trainer) connected to a screen. The screen displays various routes which the participant can select and this mimics the experience of cycling outside, thus offering simultaneous physical and cognitive stimulation.
Positive effects in favour of exergaming were found on cognition and social functioning in people with dementia and on carers’ distress related to their relative’s neuropsychiatric symptoms and the carers’ sense of competence. Furthermore, persons with dementia, family carers and staff were satisfied with the exergaming intervention.
Exergaming can thus be considered a meaningful activity, and a good alternative when outdoor physical activities are not possible because of weather conditions or safety risks (fall incidents, wandering).
Read more >
Guidance
When persons with dementia use technology for meaningful activities this may not only impact their own quality of life but also the well-being of their (primary) family carers.
Explanation and example
In the exergaming project, people with dementia were engaged in an exergaming activity or activities as usual in day care centres. We studied the effects on persons with dementia as well as on their family carers. In carers, positive effects were found in favour of the exergaming intervention, i.e. on the carers’ distress related to their relative’s neuropsychiatric symptoms and the carers’ sense of competence (after a three months intervention period).
Read more >
Guidance
Methodological sound effectiveness research into eHealth interventions for community dwelling persons with dementia is growing. To determine the added value of such interventions, it is important to look at their effects and costs. This gives a balanced picture and helps policy makers to make the right decisions when deploying eHealth interventions.
Explanation and example
Positive effects were found of exergaming compared to usual activities in day care centres. The provision of exergaming brought additional costs related to the equipment (purchase and maintenance) and staff involvement. Compared to non-technology based interventions, especially equipment costs can be a cost driver.
In the exergaming study, the participating organisations received a list of potential funders for the equipment to be used, and various funding organisations (charitable organizations) were willing to pay for it. In some cases this helped to participate in the study.
Taking into account the intervention costs may help day care centres to balance the positive effects of using the eHealth interventions (for people with dementia and their carers) against the long-term costs (to be covered by own funding or external funding). This will promote a well-informed implementation and securing of the eHealth intervention.
Read more >
Health care technologies
Guidance
Internet training programmes for family carers have potential to increase carers’ well-being, to reduce distress, depression and anxiety symptoms and to increase knowledge skills.
Explanation and example
A systematic review (Egan et al. 2018) about online training programmes for family carers reported on two studies in which improvements in depression symptoms were demonstrated, two studies with overall improvements in anxiety and two studies showing reduction of stress symptoms. Good examples of informative websites and internet training programmes for family carers are ‘Mastery over Dementia’, iSupport, ‘iCARE: Stress management eTraining programme’ and the STAR E-Learning course.
Read more >
Social Health Domain 2: Manage ones own life and promote independence
Guidance
More high quality, ecologically valid, controlled studies must be planned, funded and executed in order to properly evaluate the effectiveness of technologies designed to be used by people with dementia and to improve social participation and self-management.
Explanation and examples
A systematic review found that in the whole world only nine controlled evaluation studies with technologies designed for people with dementia have been carried out in ecologically valid settings, to assess effectiveness in improving social participation and self-management. Controlled studies are the most effective way of conducting unbiased evaluations, from which causal inference can be drawn. Policy-makers should be demanding this level of evidence as a condition of investment in such technologies. So far, studies have been conducted with VR-based technologies, other wearable technologies, and software applications. However, only a single study was found to be of good quality. Other technologies for people with dementia have not yet been the subject of a single ecologically-valid, controlled study with these outcomes (this includes, for example, social robots). In order to conduct high quality studies, researchers must ensure that studies are adequately statistically powered based on a sufficiently large sample; include active technology-based control interventions, so that is controlled for attention; and conduct and report intention-to-treat analyses, taking into account data of all participant to the study, including dropouts, and not only those who completed the intervention. Funding bodies must recognize the need to fund such studies accordingly. Clinicians, healthcare providers, policymakers and users of technology should expect and demand that such high-quality evidence is available to support decision-making.
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
See recommendation no. 3.2.5.1
Read more >
Guidance
Low-cost pet robots are a promising technology to improve the psychosocial health of people living with dementia. More high quality studies with sufficiently large sample sizes should be conducted to properly investigate their impacts.
Explanation and examples
Pet robots are a technology-based substitute to animal assisted therapy. However, the high costs of many pet robots can hinder the use of pet robots in dementia care. A scoping review was conducted to understand the impact of using lower-cost (more affordable) pet robots. Synthesised findings from nine studies suggested that low-cost pet robots improved the communication, social interactions and other health domains of older adults and people living with dementia. However, most studies had a small sample size and were of varying quality. Moving forward, more rigorous studies are necessary to investigate their impacts.
Read more >
Guidance
Low-cost pet robots demonstrate the potential to positively impact the psychosocial health of people with dementia and their caregivers. Due to their lower cost, they may be more accessible and affordable and should therefore be considered for use in dementia care.
Explanation and examples
Although pet robots have demonstrated positive impacts on the wellbeing of people with dementia, their affordability can impede their uptake in dementia care. A scoping review, content analysis of consumer reviews and a qualitative study showed that the impacts of low-cost pet robots on people with dementia resembled the effects of other higher costed (but more advanced) pet robots. These included improved mood, companionship, increased activity engagement and reduced anxiety. Caregivers also experienced knock-on effects, such as feelings of joy and relief. Low-cost pet robots are more widely accessible to the public since they can be purchased off-the-shelf. While promising, findings of their positive impacts are subject to bias. More rigorous studies are necessary to confirm their impacts.
Read more >
Guidance
Care providers should consider providing people with mild cognitive impairment (MCI) or mild dementia with the FindMyApps tablet-based intervention, or even a usual tablet without FindMyApps if accompanied with appropriate training, as an effective way of improving their social participation.
Explanation and Examples:
Evidence from the FindMyApps project has identified increases in social participation associated with use of the tablet-based FindMyApps intervention or a usual tablet without FindMyApps, when accompanied by appropriate training. The improvements were slightly more pronounced with the FindMyApps intervention than with a tablet without FindMyApps, particularly with respect to the diversity of social activities in which people participated (as opposed to the overall frequency of social activities). Evidence was also found for people with MCI/mild dementia experiencing apathy prior to receiving the interventions having better quality of life outcomes when they received FindMyApps. All improvements found were small.
Caregivers’ sense of competence refers to how well caregivers feel they can provide care for their family member with dementia or friend, and for how long. Evidence from the FindMyApps project has identified that the FindMyApps intervention is associated with a greater sense of competence for caregivers (moderate effect size) of community-dwelling people with MCI/mild dementia than a normal tablet and should therefore be implemented by preference to a normal tablet.
Read more >
Technology in everyday life
Guidance
Consider involving occupational therapists in providing interventions that enable people with dementia to use the everyday information and communication technologies they have.
Explanation and Examples
A standardized questionnaire mapped how many Everyday Information & Communication Technologies (EICT) (maximum 31) were relevant to 35 people living with dementia and 34 people with no known cognitive impairment in Sweden. A relevant EICT is one that is being used, or has been used in the past, or is planned for use in future. The median amount of relevant EICTs was shown to be 11 in the group without dementia, and 7 (significantly less) in the group with dementia. Each person also rated their ability to use (maximum 90) relevant Everyday Technologies (ETs) on a 5 step rating scale. This data was analysed (in a Rasch model) to produce a score for each person’s ability to use ET. When we compared ability to use ET with amount of relevant ETs in each group, the more EICTs a person counts as relevant, the higher was their ability to use ET. This pattern was only found in the group of people with dementia, and not the group without. The amount of relevant EICTs is affected by a person’s ability to use them. So some people may need support to identify the usefulness and possibility to use an EICT function that they have access to.
Read more >
Technology for meaningful activities
Guidance
Exergaming in day care centres can be implemented more successfully by making more than one employee responsible for it.
Explanation and examples
We have asked day-care centres for people living with dementia, which factors were important for successful implementation of Exergaming. Sometimes, only one person in the day-care centre was responsible for the Exergaming activity. If this person was not at the day-care centre, because he/she was ill or left for another job, the Exergaming activity often was forgotten.
Read more >
Guidance
Employees of care organisations should be supported by the management in their responsibility for Exergaming as a new activity. Managers should be actively engaged in Exergaming and be kept updated on any developments with regard to Exergaming (i.e. positive experiences of people with dementia practising Exergaming, any potential issues with the activity).
Explanation and examples
We have asked day-care centres for people living with dementia, which factors played a role in successful implementation of Exergaming. The staff of these day-care centres sometimes did not feel supported by the management in supervising and implementing the Exergaming activity. This made it less likely for them to implement it.
Read more >
Guidance
Introduce new application (app) technology to a person with dementia by focusing on aspects that are likely to encourage their interest, such as family photographs, video calls with friends and family, music, games, or art applications.
Explanation
This guidance is based on a review of the literature on the use of touchscreen technology by people with dementia and carers.
Read more >
Guidance
Internet should be freely available in care homes so residents with and without dementia can have access to online resources (e.g.social media, entertainment, information).
Evidence
The multi-country survey indicates that it is not common for the residents to have access to the internet in care homes, with the internet use restricted to the staff. This means that many social and leisure activities based on ICT will be inaccessible for people with dementia, depriving them of enjoyable, meaningful activities and social networks.
Read more >
Health care technologies
Guidance
People involved in the provision of support to family carers, such as health professionals, patient organizations, should inform them about the potential benefits derived from the use of online interventions and actively promote their use.
Explanation and example
Despite the potential benefits of Internet carer support and training programmes, family carers are not always informed about the existence and use of online alternatives to traditional face-to-face support programmes. Extra attention should be paid to inform and motivate family carers to start and continue using Internet training programmes, especially in countries where the use of the Internet for health related purposes is not common yet. India trial (Mehta et al. 2018) Rrecruitment and adherence for a randomized controlled trial of an online support programme in India (Mehta et al. 2018) turned out to be challenging as most of the family carers were not accustomed to access to the Internet for health-related reasons.
Read more >
Guidance
To make complex health technologies more useful and applicable for users, it is crucial to involve all users, including staff, in the early phase of development of these interventions.
Explanation
In developing complex health technologies that would be delivered by nursing staff to people with dementia, it is important to involve the nursing staff themselves in the early phase of development of such technologies. In doing so, complex health technologies can be more useful and applicable for the nursing staff.
Read more >
Guidance
To better implement complex health technologies in complex settings such as nursing homes, it is important to make these health technologies flexible to existing situations and processes including: the specific context of the nursing homes; the needs and roles of nursing staff; and the timing and order of implementation of different intervention components (e.g. training on specific subjects).
Explanation
Nursing homes may have their own culture and own ways of working. Hence, complex health technologies should be able to fit in this context. The nursing staff may also have varying levels of knowledge and skills and complex health technologies should be flexible for tailoring so that it can be used based on the capabilities of all nursing staff. The timing and order of implementing components of the complex health technologies may not be applicable in all situations, so interventions should be flexible for nursing staff to decide when to implement certain complex health technology components.
Read more >
Guidance
When implementing Advance care planning (ACP) as a complex health technology in a complex setting such as a nursing home, multiple levels should be targeted, including management, nurses, care staff, volunteers, visiting or residing physicians, families, cleaning or other staff.
Explanation
The implementation process will have a higher chance of succeeding when multiple levels are targeted within the nursing home. Colleagues in the nursing home can help each other to implement the intervention, creating a positive and open environment to learn and develop new skills and deliver the best care possible. In this way the intervention can produce a shift in working culture and attitudes and deliver sustainable change.
Example
The ACP+ intervention targeted not only the (head) nurses, but also other care staff and cleaning, kitchen and maintenance staff. Also, engagement of the management was required for participation in the trial. A few highly motivated people were extensively trained in conducting ACP conversations and this knowledge was past onwards to colleagues via internal training sessions. In this way the whole nursing home was involved in the intervention, leading to greater participation of all nursing home employees.
Read more >
Guidance
Issues such as access to the EPR system, appropriate training and system development and support should all be considered by nursing homes before and during the implementation of EPR systems.
Explanation and Examples
Access or non-access to various parts of the EPR system should be discussed and put in place. For instance, management should consider whether auxiliary staff should be allowed to access medical information, such as dementia diagnosis, and whether this would consequently entail training in the field of dementia. Appropriate training in the EPR system according to individual staff needs is also required, as some staff may be more experienced in the use of technology than others. Training ‘on the job’ was found to be preferred by many over classroom-based teaching. Finally, software developers should consider working alongside nursing homes during the design of EPR systems in order to ensure software is appropriate for their needs. Developers should continue to be involved in improving the EPR following implementation, as part of an iterative cycle.
Read more >
Guidance
Occupational therapists must adopt telehealth practices as a supplement to in-person occupational therapy to avoid service disruption in times of crisis. This requires legislation and public promotion, clear strategies and guidelines for health service managers, and finally, training and continuous support for end-users.
Explanation and Examples
A global online needs-assessment survey among occupational therapists was undertaken to determine the impact of the COVID-19 pandemic on telehealth practices in occupational therapy worldwide and to get insight into facilitators and barriers in utilising this form of service delivery. The survey was circulated in the occupational therapy community by the World Federation of Occupational Therapists (WFOT) between April and July 2020, collecting responses to closed-ended questions, in addition to free-text comments. 2750 individual responses from 100 countries were received. The results revealed a significant increase in the use of telehealth strategies during COVID-19, with many reported benefits. Occupational therapists who used telehealth were more likely to score higher feelings of safety and positive work morale and perceived their employer’s expectations to be reasonable. Restricted access to technology, limitations of remote practice, funding issues and slow pace of change were identified as barriers for some respondents to utilising telehealth. Facilitators included availability of supportive policy, guidelines and strategies, in addition to education and training.
Read more >
Guidance
To provide high-quality elderly and dementia care, Digital Health Technologies (DHTs) can potentially help achieve the full capacity of Comprehensive Geriatric Assessments (CGAs). In addition they can improve communication and data transfer on patients’ medical and treatment plan information between care settings and stakeholders as well as improve health decision-making. Finally, they can help to share the responsibility of the geriatric assessment between professionals, thereby avoiding overloading the workload of individual users and reducing their psychological stress.
Explanation and Examples:
Due to the higher rate of transitions between care settings in older populations, associated with the complexity of an ageing population and the shift from institutional care to home care, CGAs have become an important assessment tool as they encompass multiple domains and address the variety of complex problems in frail older people. They are considered as multidimensional assessments, using quantitative assessment scales, that support multidisciplinary care teams in clinical decision-making and personalized care planning to meet the needs of older people, their families and carers, focusing on functional status and quality of life.
However, to reach the full potential of CGAs, their implementation should be supported by electronic data systems, which provide relevant outputs and allow timely sharing of information within multidisciplinary teams of healthcare professionals and between different healthcare settings. The use of DHTs can potentially help them reach their full capacity and overcome the data transfer limitations between care settings and stakeholders. To improve the usability and implementation of these DHTs, the following features are recommended: a) accessibility of individual assessment by multiple healthcare professionals and the possibility of splitting sections according to professional expertise to share responsibility for assessments; b) the use of secure data storage, such as clouds; c) automatization of real-time calculation of scales and outcomes with a graphical representation of the person’s profile and health status; d) automatic alerts, notifications and continuous monitoring of item completion; and e) provision of personalized care plans according to the data collected.
Well-designed digital health technologies can contribute to the safety of the potential users (e.g. healthcare professionals and stakeholders) and reduce psychological stress, including burnout and low morale, by avoiding overloading the workload of healthcare professionals. For example, by sharing the responsibility for carrying out the assessments between different professionals.
Read more >
Social Health Domain 1: Fulfill ones potential and obligations
Guidance
Health and social care professionals working with people with Young Onset Dementia should clearly signpost to online peer support services, to help people find the support they need.
Explanation and Examples
Peer support can be highly beneficial for people with Young Onset Dementia and make the post-diagnostic period more positive. It can contribute to different aspects of social health: their ability to fulfill one’s potential and obligations, management of their own life and participation in social activities. People can share experiences, information, and coping skills in these areas. This goes beyond support that health and social care professionals, or friends and family can give. Given these benefits, peer support should be accessible to every person living with Young Onset Dementia. However, access to specialised (support) services varies widely across the UK. Therefore, online peer support could offer a solution.
Our research showed that people with Young Onset Dementia experienced a severe lack of support and signposting to (peer) support services. Benefits of having peer support online included not having to travel, not having the sensory overload of being in a room full of people, and finding it comfortable to join from their own home. Having their support group gave many of them hope again, and some called it their lifeline. Our online survey showed that the main reason why people did not use online peer support was that they did not know it existed, or they did not know where to look for support. Some of those who did not have experience with online peer support would be interested if they knew where to find it. This indicates a need for professionals to clearly signpost to (online) peer support services and information.
Read more >
Guidance
Online peer support groups on text-based platforms, such as Facebook groups or discussion forums, can have a much larger membership than in-person groups or groups using videoconferencing platforms. Moderators should provide a clear description of the purpose of the group and who it is for, and what the ground rules are.
Explanation and Examples
Findings from an extensive systematic literature research on online peer support for people with different chronic, neurodegenerative conditions, identified several elements of best practice. Online health communities, for example on social media or discussion forums can have a large membership and tend to be more anonymous in nature. To prevent access by people for whom the group is not really intended, the group should be closed. This means that the moderators need to approve before new members can join. This goes hand in hand with the purpose of the group and who it is for. For example, if the group is only for people living with a Young Onset Dementia diagnosis, moderators may want to avoid that family members, healthcare professionals, or researchers access the group. This is to allow the members to speak freely and to respect their privacy. It is also important to clearly indicate, preferably on the home page, who the group is for. Is it only for people with a diagnosis, only for carers, or for both? Finally, it is the responsibility of the moderator to intervene when someone shares harmful, misleading, or disrespectful content in the group. The moderator should delete such messages and, if possible, contact the author. In this way the moderator ensures the group remains a safe space for everyone.
The findings of the systematic literature review were echoed by people with Young Onset Dementia who took part in individual interviews and had experiences with peer support on text-based platforms.
Read more >
Social Health Domain 2: Manage ones own life and promote independence
Guidance
See recommendation no. 3.3.4.1
Read more >
Guidance
See recommendation no. 3.3.4.2
Read more >
Guidance
While designing social assistive robots the following recommended features should be considered to promote successful implementation: low-cost affordable design (pet robot is preferred to humanoid), language mutation for target user and integration with Smart Home IoT (including IoT security mechanisms). During the development phase co-creation should be promoted.
Explanation and Examples:
These recommendations are based on the main findings of a scoping review. The scoping review investigated the state-of-the-art in social assistive robotics, i.e. the current technological advances towards a single framework for effective, safe and secure implementation of social robots for people with dementia. The scoping review qualitatively examined the literature on the use of companion robots, including both pet-like and humanoid robots, and Internet-of-Things (IoT) security, coupled with the new 5G technology for home-based elder care. A comprehensive search strategy was developed and selected databases were looked through with relevant keywords. From the 355 full-text articles found, 90 articles were selected to be examined. In order to ascertain the operation of social assistive robots in the future, remaining challenges, unused opportunities, security risks and suggested remedies are discussed, and a dementia-centred concept and implementation framework proposed.
The following set of recommendations were formulated based on the main findings:
- Consider using a pet robot instead of a humanoid assistive robot as the high cost of the latter for a similar impact and user acceptance cannot be justified.
- Consider low-cost, affordable design and various language mutations for wider deployment in practice, thus allowing more comparative studies, which could provide convincing arguments for using the robot.
- Integrate robot with Smart Home IoT to enhance its functionality towards managing ones own life and promote independence.
- Consider data security, and especially IoT security, prevention mechanisms while integrating the social robot with IoT smart home sensorics.
- Promote wider user involvement and higher level of participation (co-creation) in the development phase of the robot.
- Introduce clearly, and particularly identify, the concerns and needs of people with dementia in the design process.
- List the potential risks and misuses of IoT vulnerabilities, including their remedies, in the design process.
Read more >
Guidance
Social media have the potential to be an additional supportive medium for people with dementia. It is recommended to signpost individuals with dementia to social media platforms to leverage their potential.
Explanation and Examples:
We conducted an online survey with 143 people with dementia to explore how they used social media platforms and what kind of information they shared on their accounts. Our findings show that people with dementia use various different social media platforms like Facebook or Twitter to raise awareness, give and receive support, and to share their experiences of living with dementia. As subsequent older generations will use technology more and, consequently, will become more tech-savvy, social media platforms will become more relevant for this population. As post-diagnostic support is often lacking, social media platforms can be used as medium that is widely available and easily accessible to offer people with dementia additional (peer) support. Examples of these platforms include online forums like Talking Point by the Alzheimer’s Society UK, Facebook groups run by charities or dementia organisations, or Twitter where many people with dementia are active. Signposting people with dementia to these social media platforms is therefore recommended.
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
Understanding how social robots positively impact nursing home residents as well as analysing practical challenges are important when implementing robotic assistive technology in nursing homes
Explanation and examples
An important facilitating factor to the acceptance of social robots in nursing homes is understanding and seeing how social robots positively impact residents, for example by improving the communication, decreasing loneliness, providing joy to residents, calming agitated residents or generally increasing their wellbeing. Understanding these benefits will facilitate the acceptance of social robots by staff as well as by relatives, but is also important for the resident to accept the social robot, as their acceptance will be influenced by the views and attitudes of staff and relatives.
On the other hand, one of the key hindering factors to the acceptance of social robots in nursing homes are practicalities of everyday life in the nursing home, such as storage, hygiene, finding a quiet place, scheduling time for robot use or the need to charge the robot.
We conclude, that applying an acceptance model of social robots (here the Almere Model) is an interesting and feasible way to trace facilitators and barriers of implementation of social technology in nursing homes, where involvement in social activities and enhancing positive experiences are important foci of interventions to improve social health.
Read more >
Guidance
Technology developers and researchers should be aware of the different contextual factors that can affect the translation of research on social robots to real-world use.
Explanation and examples
Barriers and facilitators affecting the implementation of social robots can occur at different levels. For example, they relate to the social robots’ features, or relate to organisational factors or external policies. A scoping review was conducted to understand the barriers and facilitators to the implementation of social robots for older adults and people living with dementia. 53 studies were included in this review. Most existing studies have disproportionately focused on understanding barriers and facilitators relating to the social robots, such as their ease of use. However, there is significantly less research that has been conducted to understand organisational factors or wider contextual factors that can affect their implementation in real-world practice. Future research should pay more attention to investigating the contextual factors, using an implementation framework, to identify barriers and facilitators on different levels to guide the further implementation of social robots.
Read more >
Guidance
Implementing assistive technology could be promising in long-term care to address loneliness in dementia, but further studies are needed to tailor assistive technology to people living with dementia in different care settings and to investigate its effect on loneliness.
Explanation and examples
Active & Assisted Living (AAL) technology aims to support coping with the consequences of dementia. A scoping review was conducted to learn if and how AAL addresses loneliness in people living with dementia in long-term care. Although, only one study focused directly on the impact of AAL technology on loneliness, findings suggest that AAL were used in the context of psychosocial interventions and proved to have had an impact on loneliness in people living with dementia. It remains unclear why loneliness was almost never included as an outcome in technology studies. Since we were not able to derive clear effects of assistive technology on loneliness from the included studies, we recommend using loneliness outcome measures in future intervention studies into AAL technology.
Read more >
Guidance
See recommendation no. 3.3.4.1
Read more >
Guidance
See recommendation no. 3.3.4.2
Read more >
Guidance
Technological solutions that can safeguard the social health of nursing home residents with dementia should be implemented as an integrated part of caregiving procedures. This requires formally incorporated technology guidelines and continuous training of staff. As developing and implementing technology to promote social participation faces substantial barriers as long as social health is not recognized on equal terms as the physical and mental health domains, first, social health needs to be acknowledged as a priority which requires major efforts at the societal-, organizational and individual levels.
Explanation and examples
Cross-sectional data from a national online survey conducted among German nursing homes, on the impact of the COVID-19 pandemic, showed that efforts were made to ensure social participation among residents with dementia, and the use of technology in doing so.A large proportion of respondents observed an increase in at least one Behavioural and Psychological Symptom in Dementia (BPSD) in residents with dementia. Many reported that social activities in the nursing home were cancelled, which was due to COVID-19 cases and staff shortages from 5 % and up, revealing just how easily neglectable social health strategies in nursing homes are. Half of all respondents reported having had no formal training in the use of social technology to engage their residents with dementia. Although more than 70% had provided opportunities for using technology for social purposes, the low frequency of established procedures seems to indicate ad hoc solutions to ensure the social health of residents with dementia.
At the micro-, meso- and macro level requirements were identified to promote social participation using technology. These requirements revealed that integrating technological solutions in institutional settings, requires efforts at individual-, organisational and societal level.
Read more >
Guidance
To minimise potential distress and negative impacts from using pet robots, researchers and care providers should assess their suitability for individuals with dementia, and facilitate their use based on each individual’s preference, needs and abilities. As the needs of people with dementia can fluctuate, care providers should also monitor and re-evaluate the use of pet robots.
Explanation and examples
Findings from a scoping review of eight studies showed that some people with dementia did not respond to pet robots. Some had negative responses such as agitation, or became jealous when the robot was shared with other residents in care facilities. An analysis of 1,327 consumer reviews on a low-cost robotic cat showed similar findings. Likewise, interviews with care providers from nursing homes revealed that they had similar experiences. To minimise the risks of potential negative impacts, the use of pet robots for each individual has to be carefully considered. This should encompass:
-
Assessment
Assess the individual’s preferences, needs, functional abilities and needs (e.g. occupational needs, and physical, cognitive, and sensory abilities). If used in a care setting, consider discussing the use of pet robots with family members.
-
Facilitation and Tailoring
Based on the assessment, provide facilitation or tailored support to individuals. For example, if the individual has difficulties initiating interactions with the pet robot, consider providing assistance
-
Monitoring & Evaluating
Monitor and evaluate the individual’s reaction to pet robots, and intervene if the individual shows signs of distress. These observations should be shared with and discussed with other care providers if used in care facilities
Read more >
Guidance
Residents with dementia and their family members should be involved when planning to introduce pet robots in long-term care settings and when using pet robots.
Explanation and examples
In a consensus-building exercise involving 56 international experts (care professionals, organisational leaders and researchers), experts established the importance of including residents with dementia and their family in the implementation of pet robots in long-term care facilities. When planning to adopt pet robots in long-term care facilities, the opinions of residents with dementia and their family members must be sought. Examples include
- Seeking their opinions on which pet robot to purchase by showing them different pet robots, and asking or observing their reactions to each robot
- Seeking feedback on their preferred ways of using robots, such as whether they prefer the robots to be individualised or shared with other residents.
When using pet robots, residents with dementia and their family members must be supported to be actively involved. For example:
- Residents may be involved in “taking care” of robots.
- Family members could provide support or use the robots as topics of conversations during visits.
Read more >
Guidance
Before introducing pet robots in a long-term care facility, consensus discussions among stakeholders, such as care professionals and managers, should be conducted, to discuss whether (and why) pet robots should or should not be introduced for residents with dementia. In addition, the facility’s readiness to introduce pet robots should be carefully considered.
Explanation and examples
In a modified Delphi study involving 56 international experts (care professionals, organisational leaders and researchers), experts agreed that these strategies are critical to support the implementation of pet robots in long-term care facilities. Consensus discussions should involve all care providers who may be directly or indirectly involved in the care of residents with dementia. Examples of discussions may include:
- The importance of bringing in/using pet robots to address a chosen problem (e.g. to address residents’ needs or support care staff in their delivery of care for residents with dementia)
- Appropriateness of using pet robots to address the problem(s), such as whether they align with workflows.
In addition, the organisation’s readiness to implement pet robots should also be assessed. Examples include:
- Assessment of financial resources
- Assessment of manpower and logistical resources (e.g. sufficient space and charging point).
Read more >
Guidance
Care staff should be educated about the use of pet robots in dementia care through educational meetings that are tailored to the needs of different staff. In addition, they should be provided with ongoing trainings to support them in applying this knowledge as part of their delivery of dementia care.
Explanation and examples
In a modified Delphi study involving 56 international experts (care professionals, organisational leaders and researchers), educational meetings and ongoing trainings are identified as critical strategies to support the implementation of pet robots in long-term care facilities. The purpose of conducting educational meetings is to provide care staff with overall knowledge on the role of pet robots for dementia care. Such sessions should be tailored to the different needs of each care professional. Examples of content may include:
- Evidence supporting the use of pet robots in dementia care, such as information about their impacts on residents, who may benefit and who may be at risk of distress
- How pet robots can support caregiving
While the purpose of education is to provide overall knowledge about pet robots, the purpose of conducting ongoing training is to support care professionals to acquire practical skills and confidence to use pet robots in dementia care giving. Examples include:
- On-the-job training
- Structured supervision
- Training based on each staff experiences/knowledge.
Read more >
Guidance
The cost of pet robots can prohibit their uptake in long-term care facilities for dementia care. There may also be additional costs involved in implementing pet robots, such as manpower and time related costs. Different funding sources need to be considered to acquire sufficient funding to support the implementation effort.
Explanation and examples
In a qualitative study involving 22 care providers from nursing homes, the cost of purchasing pet robots have been reported as a concern. Some care providers reported the use of charity funds to support the purchase of pet robots. In a modified Delphi study, experts (care professionals, organisational leaders and researchers) established that it is necessary to creatively seek and acquire funding to support the implementation of pet robots in long-term care facilities. Examples of potential funding sources may include:
- Existing funding resources
- Raising private funds (such as donations or charity)
- Shifting or (re)prioritising the use of funds within the organisation based on their impact on people with dementia
The funds may be used to support different aspects of implementation. Examples include:
- Fund the introduction and adoption of pet robots
- Support other time limited actions needed for initial implementation, such as purchasing cleaning materials
- Training (e.g. developing educational materials)
Read more >
Guidance
There are many considerations when planning to implement technological interventions. The issues can be grouped into context, implementation and mechanism of impact factors. Evidence from the FindMyApps project has identified, within these categories, specific factors that are important for successful implementation of a tablet-based intervention, such as FindMyApps. Potential tablet-users and care providers are advised to base their decisions on this evidence.
Explanation/examples:
The FindMyApps project compared the FindMyApps intervention to usual tablet use by community-dwelling people with mild cognitive impairment (MCI) or mild dementia. The following factors were identified as influencing the success of implementation of both the FindMyApps intervention and a standard tablet:
- Context:
- People with MCI/mild dementia who previously used a tablet are more likely to use the intervention. Intensive one-on-one support is recommended to those who have never used a tablet.
- People with MCI and younger people with MCI/mild dementia may use the intervention more. Extra support is recommended for older people with dementia.
- People experiencing apathy may benefit more from dementia-specific tablet programmes, such as FindMyApps, which provide easy access to selected apps, than from a standard tablet.
- Implementation:
- People with slower Wi-Fi connections may find the tablet harder to use.
- It is often feasible to provide support by telephone and/or video-call but face-to-face contact is more suitable for those who have never used a tablet before.
- Few people use passive support, such as a telephone helpdesk. It is therefore recommended to pro-actively offer support to those who may need it (see above).
- Mechanisms of impact:
- Tablet-use may support social contact and engagement in meaningful activities, more than instrumental activities of daily living. It is recommended to set personal goals accordingly.
- Limitations of specific tablet-apps (e.g. pop-up advertising, requirements for user-accounts with passwords) should be considered.
- The quality of tablet-use, seems more important for social health than the quantity (frequency of duration) of tablet use. Set personal goals and evaluate accordingly.
Read more >
Guidance
See recommendation no. 3.3.5.5
Read more >
Guidance
See recommendation no. 3.3.4.4
Read more >










 As the INDUCT project manager, most of my tasks have been ‘behind the scenes’. I have been responsible for submitting scientific deliverables, writing reports for the funder, negotiating deadlines and updating the EU Portal. A project manager functions as a middleman between the EC Project Officer, beneficiaries, partners and ESRs.
As the INDUCT project manager, most of my tasks have been ‘behind the scenes’. I have been responsible for submitting scientific deliverables, writing reports for the funder, negotiating deadlines and updating the EU Portal. A project manager functions as a middleman between the EC Project Officer, beneficiaries, partners and ESRs.