Technology in everyday life
Guidance
During the development or use of technological devices, the individual needs of the person with cognitive impairments (e.g. dementia or MCI) and carer should be considered. This includes not only everyday technology, but also surveillance technology (ST) and technology used during cognitive training sessions. Increased awareness and offered assistance is recommended.
Explanation and Examples
People with dementia tend to face more and other difficulties than people with MCI when using relevant everyday technologies such as cash machines, calling or texting with a cell phone or using a DVD player, and thus need more assistance in technology use. This may also be the case with ST and technology used for cognitive training.
For example, ST are often presented as a neutral technology, which enables carers to minimise risk. However, the views of users have not been sought by ST developers, which limits the usefulness of ST and suggests the need for the empowerment of user groups. Therefore, a study of audience reception was undertaken through focus groups, online discussions (Netherlands) and PPI (UK). Hereby people with dementia could speak for themselves, which has allowed their needs to be compared with carers. There was no clear recognition that such needs differed between people with dementia and carers, and it has not previously been recognized that this leads to a mismatch between a user’s situation and the product design and how this plays out in the acceptance and use of ST. Although, carers and people with dementia have not yet reached an agreement on the privacy debate and on how the media should portray dementia, it is clear that carers often tamper with ST to make up for a lack in current designs. The results suggest that ST are being resold or rebranded by providers to use for dementia, whilst users may experience physical and cognitive barriers to using such technologies for safety reasons.
Regarding technology for cognitive training: As older people have little experience with technological devices, and so may experience problems, professionals involved in cognitive training should monitor training sessions from the outset. The professional must observe and ensure the ability of the older person to understand the instructions given through the technological device, so that the person can really benefit from the cognitive training by computer. For example, in sessions with GRADIOR, a cognitive rehabilitation program, there is always a professional in charge who helps older people to understand the exercises they may experience difficulty with.
Read more >
Guidance
Public health policy should more fully consider the undesired side effects of dementia prevention technologies and discourses which may reinforce the fear of dementia and imply a moral responsibility on people who cannot maintain cognition in later life due to the progression of the condition.
Explanation and Examples
A review of the literature shows there is little evidence for the effectiveness of brain training to prevent dementia. Furthermore, ethnographic research has generated evidence that engagement with it can act as a form of social exclusion by separating older people into those who have ‘successfully cognitively aged’ and those who have not. Indeed, the promotion of this technology implies an individual responsibility to stay cognitively healthy, implicitly reinforcing anxiety and blame around the condition and people who live with it. These side effects can reinforce the exclusion of people with the condition.
Read more >
Health care technologies
Guidance
To improve usability design of the technology should be developed specifically on the characteristics of the person with dementia, with respect to vision, auditory and cognitive capacities.
Explanation and Examples
Dementia is mainly suffered by elderly people. It´s well known the visual and auditorily perception changes. Shapes, colours, glares, temporal frequency of stimuli, visual acuity, and relevant visual stimuli can be bad perceived. Therefore, the design of any technology should be focused and fitted to these perceptual changes. Consequently, it is important to increase the lighting of the context of the task, the level of contrast and font size.
Equally elderly people might suffer impaired hearing, especially in sensitivity to high frequencies, discrimination of tones and differentiation of the speech of the background noise. Therefore, it is necessary for any technology to increase the intensity of the stimuli, control the background noise, avoid stimuli with high frequencies and adapt the speed of the words.
The design of the technology should take into account the cognitive impairment of a person with dementia (type, level, and deficits associated with impairment). Technology for rehabilitation must comprise different difficulty levels, take slow processing speed into account by extending response intervals of exercises, and an increase the variety in types of exercises.
The degree of usability of a technology will influence the user´s experience, generating a degree of satisfaction in the person with dementia that will affect their level of motivation to continue using a rehabilitation program such as Gradior.
Read more >
Guidance
User-centered design should be considered in the development of any technology or computer-based program for cognitive rehabilitation in people with dementia.
Explanation and Examples
User-centered design is a methodology applied in the development of programs or new technologies for cognitive rehabilitation in people with dementia. This design takes into account the target population from the beginning to the end of the development process, with the aim of investigating their needs and expectations, developing a prototype that meets these needs and evaluating the final prototype based on usability and user experience criteria.
Read more >
Social Health Domain 1: Fulfill ones potential and obligations
Guidance
To better understand how digital Patient and Public Involvement (e-PPI) and blended approaches (hybrid digital and face-to-face PPI) in dementia research can be better facilitated, it is recommended to use the E-nabling Digital Co-production framework.
Explanation and Examples
Qualitative research showed that the E-nabling Digital Co-production framework (see Figure 1) is useful for researchers, PPI coordinators and public contributors in advancing understanding of the challenges and opportunities provided by e-PPI and blended (hybrid) approaches. The framework explores preferences and implications of using different modalities of PPI and it can be useful for specific populations and contexts, for example in dementia technology research.
In this context, e-PPI needs to optimise engagement by taking into account participants’ abilities to remember instructions on how to join the e-meeting, their levels of attention and concentration, or the need for explicit cues to the speaker. The level of support must be determined which requires specialised training for facilitators or additional supporters during the meeting.
Facilitators should be aware that online meetings may deprive caregivers of respite and support that would be present face-to-face, and may exclude those who live alone or need more support.
Some of the opportunities of e-PPI are related to removing geographical constraints allowing wider participation and saving resources in terms of time, not having to travel to meetings, arrange venues, catering or other coordination such as transporting PPI representatives.
Read more >
Guidance
Digital Patient and Public Involvement (e-PPI) provides opportunities, for example, in terms of saving time, not having to travel to meetings, and fewer organizational tasks, such as transporting PPI representatives to the meeting venue. However, to optimize digital Patient and Public Involvement (e-PPI) in dementia research, technological, involvement ability, resources and ethical and welfare conditions should be taken into account.
Explanation and Examples
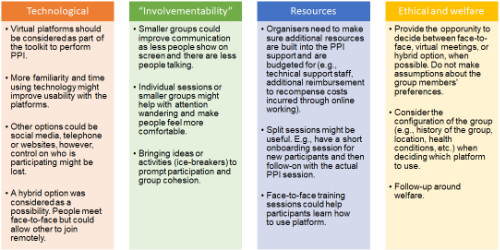
When applying digital PPI in dementia research it is important to consider four key areas of conditions. Taking these areas into account will allow identifying improvements that can be made to e-PPI to make it more effective and efficient, and problems avoided (see also Figure 2):
-
Technological: refers to constraints, preferences, and opportunities of the used technology.
Improvements: virtual platforms must be considered as part of the toolkit to perform PPI; hybrid options (digital and face-to-face) must be provided.
-
Resources: is associated with personal resources such as fatigue or personal resilience; professional resources such as increased demands on conducting PPI online; and other resources such as costs of coproduction platforms, phone credit, printing, software, or budget for more frequent meetings.
Improvements: make sure additional resources are included such as technical support staff or reimbursements for online meeting costs; face-to-face training could help participants to learn how to use the platform.
-
Involvementability: refers to requirements that are related to the success of a design task or process. How involvement differs in a digital space or how it can be translated to different populations online.
Improvements: smaller groups can help prevent attention wandering; limit the number of people on the screen.
-
Ethical and welfare: describes aspects such as the welfare of public contributors (people with dementia and caregivers), digital exclusion, impact on social communication, data security, etc.
Improvements: consider the configuration and history of the group when choosing which platform and approach (online, face-to-face or blended) to use; follow-up of public contributors’ welfare
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
People designing psychosocial interventions for people with dementia should be aware that viewing generic, rather than personal photographs, can also be a meaningful activity for the person with dementia. Moreover, viewing these photos digitally was found to be either similar to or better than viewing conventional printed photos.
Explanation and Examples
There is evidence that using generic photos, versus personal family photos, in psychosocial interventions for people living with dementia can be more effective in promoting social interaction and eliciting stories with emotional and personal significance. Generic photos may feel less threatening compared to using personal photos in conversation with the person with dementia, the conversation that arises becomes more flexible and less demanding of remembering specific people or events. This can lead to better social interaction, mood, and eventually, better quality of life for the person with dementia.
Generic photographs can be more accessible and easier to acquire, lessening the time needed to, for example, ask for and collect family photographs from relatives (if these are still available). It has the potential to be cost-effective as well (compared to other art-based activities like museum visits), and has the potential to transcend societal or cultural differences.
These benefits may be even more pronounced, when generic photos are used in a digitalized format, as previous research showed that viewing digitalized photos is similar to or better (due to the pleasurable experience of using virtual reality technology; Tominari et al., 2021; Xu & Wang et al., 2020) than viewing conventional printed photos.
Read more >
Guidance
To successfully integrate social robotic platforms in community-based dementia care, such as Meeting Centres for people with dementia and carers and daycare centres, their features and applications need to be tailored to the needs and preferences of the end-users, the dynamics of group interactions, and the Meeting Centres’ activity policies and settings.
Explanation and Examples:
Research through focus groups and interviews with stakeholders on potential facilitators and barriers in the implementation of the social robot MINI indicated that for a successful implementation of social robots in Meeting Centres and daycare centres for people with dementia, it is expected to be crucial for social robot designers and developers to consider the following recommendations to guide the design of the robotic platform:
- Evaluate the needs and preferences of the participants of Meeting Centre. Qualitative research with end-users and care professionals is essential before and during the robot development phase. This will ensure the acceptance and usefulness of the robot in such contexts.
- Given the preference for group activities in Meeting Centres over individual activities, it is crucial to integrate the robot into a group setting so that it can interact with multiple users. For example, a multi-player game could allow two or more individuals to interact with a social robot at the same time.
- Avoid designing games and quiz-like activities for use on social robots to avoid, in line with the activity policy of Meeting Centres, confronting persons with dementia with their shortcomings in activities that have high cognitive and memory function demands. Instead, fun, enjoyable, and relaxing applications and games would be most appealing and beneficial.
Read more >
Technology in everyday life
Guidance
The ecological validity and cultural context in which the technology will be implemented should be taken into account, to ensure it is applicable to the ‘real life situation’ of the person with dementia
Explanation and example
When cognitive rehabilitation is applied to people with dementia, it is necessary to consider the ecological validity of each tool or instrument used to perform cognitive rehabilitation, training or stimulation. Ecological validity is determined by the ability of those tools, instruments or techniques used for cognitive training to be transferred to the patient’s daily life. Therefore, the patient may feel that using these techniques or tools in their daily lives can bring them benefits and influence their daily life, “beyond the rehabilitation session”. For example: Gradior includes images of real objects which are well-known to the users. These objects are close to those of real life, among others: calculation exercises associated with real adult life (shopping at a supermarket), presents quizzes of daily activities (prepare a specific recipe). New technologies for rehabilitation or cognitive training should consider ecological validity as their main objective otherwise it may not be appropriate for the person with dementia who uses it.
The context is a factor that must be considered in the design of new technologies, that is, it is not enough to delimit the population and its characteristics. For example: a technology may be applied in an urban context but not necessarily in a rural one, due to the difficulties that this context may have in terms of the existence and scope of communication systems (internet connection, presence of devices, etc.).
Consequently, Gradior was developed free of contents. This means that it is easy to change the contents of the software and objects interacting with the person with dementia. In this way, it can be fitted to different environments in an easy way. It is necessary that the exercises and objects have significance to the users.
Read more >
Technology for meaningful activities
Guidance
When persons with dementia use technology for meaningful activities this may not only impact their own quality of life but also the well-being of their (primary) family carers.
Explanation and example
In the exergaming project, people with dementia were engaged in an exergaming activity or activities as usual in day care centres. We studied the effects on persons with dementia as well as on their family carers. In carers, positive effects were found in favour of the exergaming intervention, i.e. on the carers’ distress related to their relative’s neuropsychiatric symptoms and the carers’ sense of competence (after a three months intervention period).
Read more >
Guidance
Effectiveness research into eHealth interventions for community dwelling persons with dementia, often rely on information from and involvement of family carers. As they may already be (over)burdened by their caregiver tasks, participation in effectiveness research may be denied. It will be helpful to think of methods to support informal carers to participate in research.
Explanation and example
In the exergaming project, a bottleneck of participation of couples into the effectiveness study, was the refusal of family carers to participate because they were already (over)burdened. To accommodate caregivers they were offered support in filling out questionnaires and a little present to thank them for their contribution. This seems to have added slightly in the number of participants in our study. Other strategies to alleviate burden of participation in eHealth research may also be considered, like data logging or ecological momentary assessments.
Read more >
Guidance
Methodological sound effectiveness research into eHealth interventions for community dwelling persons with dementia is growing. To determine the added value of such interventions, it is important to look at their effects and costs. This gives a balanced picture and helps policy makers to make the right decisions when deploying eHealth interventions.
Explanation and example
Positive effects were found of exergaming compared to usual activities in day care centres. The provision of exergaming brought additional costs related to the equipment (purchase and maintenance) and staff involvement. Compared to non-technology based interventions, especially equipment costs can be a cost driver.
In the exergaming study, the participating organisations received a list of potential funders for the equipment to be used, and various funding organisations (charitable organizations) were willing to pay for it. In some cases this helped to participate in the study.
Taking into account the intervention costs may help day care centres to balance the positive effects of using the eHealth interventions (for people with dementia and their carers) against the long-term costs (to be covered by own funding or external funding). This will promote a well-informed implementation and securing of the eHealth intervention.
Read more >
Health care technologies
Guidance
Evaluations of the effectiveness of internet training programs should explore mechanisms of change and aspects of the intervention design, such as reliability, the type of device used and modality of the intervention.
Explanation and example
The systematic review (Egan et al 2018) of internet training support for familiy carers lacks detail about potential factors which may influence the effectiveness of online programs (i.e. type of connectivity, development of the intervention, usability, etc.). The quality of individual studies selected for the systematic review was limited as more than 50% of the studies showed incomplete data reporting, and 25% showed a selective reporting of outcomes according to the risk of bias assessment performed making the generalization of the results difficult. However, the systematic review reported improvements on carer’s mental health outcomes by internet training.
Read more >
Guidance
Analyses of the moderation effect of demographic characteristic of the carers and other characteristics of the person with dementia on the internet training programs outcomes should be encouraged.
Explanation and example
Several studies have been done to find moderators of effects of online training programs for carers of people with dementia. Some studies have demonstrated that some programs were more effective for certain subgroups of carers. However, in our analyses we could not replicate these findings. Our analyses on the effect of age, gender, level of education, relationship with the person with dementia, functional status of the person with dementia and frequency of appearance of challenging behaviour suggests that the program is equally effective for all the subgroups analysed. More research is needed before we have definitive answers. A better understanding of moderators of carers’ training programs could lead to better tailoring of programs based on the specific characteristic of the carer.
Read more >
Guidance
When evaluating adherence of people with dementia to a computer-based cognitive rehabilitation program, sociodemographic, cognitive, and psychological factors should be taken into account.
Explanation and example
When we consider evaluating the adherence of people with dementia to a computer-based program for cognitive rehabilitation, it is important to consider sociodemographic (age, sex, educational level), cognitive (memory, attention, executive function) and psychological factors (level of motivation, expectations, previous computer use).
For this purpose, a periodic evaluation will help to evaluate these factors and their relation to the amount and the time that a person spends in using a computer program for cognitive rehabilitation. In this way, significant modifications could be made to the program, so that the program meets the needs of people with dementia.
Read more >
Social Health Domain 2: Manage ones own life and promote independence
Guidance
More high quality, ecologically valid, controlled studies must be planned, funded and executed in order to properly evaluate the effectiveness of technologies designed to be used by people with dementia and to improve social participation and self-management.
Explanation and examples
A systematic review found that in the whole world only nine controlled evaluation studies with technologies designed for people with dementia have been carried out in ecologically valid settings, to assess effectiveness in improving social participation and self-management. Controlled studies are the most effective way of conducting unbiased evaluations, from which causal inference can be drawn. Policy-makers should be demanding this level of evidence as a condition of investment in such technologies. So far, studies have been conducted with VR-based technologies, other wearable technologies, and software applications. However, only a single study was found to be of good quality. Other technologies for people with dementia have not yet been the subject of a single ecologically-valid, controlled study with these outcomes (this includes, for example, social robots). In order to conduct high quality studies, researchers must ensure that studies are adequately statistically powered based on a sufficiently large sample; include active technology-based control interventions, so that is controlled for attention; and conduct and report intention-to-treat analyses, taking into account data of all participant to the study, including dropouts, and not only those who completed the intervention. Funding bodies must recognize the need to fund such studies accordingly. Clinicians, healthcare providers, policymakers and users of technology should expect and demand that such high-quality evidence is available to support decision-making.
Read more >
Guidance
Ensure that the methodology for the evaluation of social robots for older adults with and without dementia is appropriate for the purpose of the study, to strengthen the results of the study.
Explanation and examples
Social robots are seen promising for supporting daily functioning and promoting overall social health of cognitively impaired older people, particularly those with dementia. Our scoping review into methodologies used to study the feasibility, usability, efficacy, and effectiveness of social robots for elderly adults with and without dementia showed that, despite promising results, the quality of studies remains low due to various methodological limitations. We have therefore formulated recommendations focusing on different types of studies that can help future researchers develop appropriate study designs to evaluate social robots, allowing for more reliable information on study outcomes:
- For feasibility and usability studies an experimental design with mixed-methods of data collection (qualitative and quantitative) are recommended. Multiple interaction sessions with the social robot are recommended as they may reveal changes in feasibility and usability, when the novelty effect gradually fades and people get used to the robot.
- Appropriate designs for efficacy and effectiveness studies are RCTs, or quasi-experimental designs when randomization is not feasible. Sample sizes should be sufficiently large, and individual interaction sessions with the social robot running for more than one month would serve best for such studies to obtain relatively robust and reliable results. Efficacy and effectiveness should only be studied in fully functioning social robots.
- It is strongly recommended not to combine different aims in one study. The preferred designs to study the feasibility and usability of a social robot, differ significantly from the designs needed to study efficacy or effectiveness.
Read more >
Guidance
Researchers interested in Social health in dementia need to develop instruments to measure the self-management aspect of Social health. Self-management is clearly defined as one of the three domains of Social health besides the capacity to fulfil one’s potential and social participation. Whilst several instruments have been proposed for the measurement of self-management, all have limitations e.g. not measuring the construct as understood in the context of Social health (managing one’s own life), being too burdensome for participants, or ceiling effects on scale of total scores. Instruments which measure the construct of self-management, as understood in this context, without burdening participants and with sufficient discriminatory power for use in intervention studies are needed in order to effectively evaluate interventions aiming to improve Social health in dementia.
Explanation and Examples:
A review of existing instruments which may be used to measure self-management found no options specifically designed to measure the construct as understood in the context of Social health in dementia (to manage one’s own life). In the FindMyApps pilot study, the Self-Management Activities Scale (SMAS) was used, but proved too burdensome to administer. In the FindMyApps definitive randomized controlled trial, another option was used to measure self-management, the Adult Social Care Outcomes Toolkit (ASCOT), which was less burdensome but also less well-aligned to the construct. The usefulness of the ASCOT proved to be further limited by ceiling effects when used in the population participating in this intervention study (people with MCI or mild dementia). Research should be undertaken to confirm consensus amongst people with dementia, their caregivers and researchers in the field on the operational definition of self-management within the context of Social health; to compose statements and scales which investigate the components of the operational definition; and to test the psychometric properties (reliability, validity, responsiveness), feasibility and discriminatory power (precision with which between- and within-subjects variation can be detected) of the resulting instrument in a population of people with MCI/mild dementia, in both an observational and interventional study setting.
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
See recommendation no. 3.2.5.1
Read more >
Health care technologies
Guidance
People involved in the provision of support to family carers, such as health professionals, patient organizations, should inform them about the potential benefits derived from the use of online interventions and actively promote their use.
Explanation and example
Despite the potential benefits of Internet carer support and training programmes, family carers are not always informed about the existence and use of online alternatives to traditional face-to-face support programmes. Extra attention should be paid to inform and motivate family carers to start and continue using Internet training programmes, especially in countries where the use of the Internet for health related purposes is not common yet. India trial (Mehta et al. 2018) Rrecruitment and adherence for a randomized controlled trial of an online support programme in India (Mehta et al. 2018) turned out to be challenging as most of the family carers were not accustomed to access to the Internet for health-related reasons.
Read more >
Guidance
To make complex health technologies more useful and applicable for users, it is crucial to involve all users, including staff, in the early phase of development of these interventions.
Explanation
In developing complex health technologies that would be delivered by nursing staff to people with dementia, it is important to involve the nursing staff themselves in the early phase of development of such technologies. In doing so, complex health technologies can be more useful and applicable for the nursing staff.
Read more >
Guidance
To better implement complex health technologies in complex settings such as nursing homes, it is important to make these health technologies flexible to existing situations and processes including: the specific context of the nursing homes; the needs and roles of nursing staff; and the timing and order of implementation of different intervention components (e.g. training on specific subjects).
Explanation
Nursing homes may have their own culture and own ways of working. Hence, complex health technologies should be able to fit in this context. The nursing staff may also have varying levels of knowledge and skills and complex health technologies should be flexible for tailoring so that it can be used based on the capabilities of all nursing staff. The timing and order of implementing components of the complex health technologies may not be applicable in all situations, so interventions should be flexible for nursing staff to decide when to implement certain complex health technology components.
Read more >
Guidance
Consider active engagement of nursing home management as a crucial component when designing complex health care technologies for nursing homes. Their commitment to the project’s success will help to ensure staff have sufficient time and other resources to participate in the new programme.
Explanation
A lack of time is one of the most important barriers for implementing advance care planning (ACP) in nursing homes. Therefore, it is crucial staff gets enough time to engage and work with the intervention in order to properly implement it. When staff is given time to spend on intervention-related tasks, instead of having to spend this time on other tasks, this will increase their ownership of the intervention.
Example
In the ACP+ programme all nursing home managers signed a contract stating they would allow their staff to spend time on the intervention. Training sessions were held during working hours and staff got paid while attending these sessions.
Read more >
Guidance
When implementing Advance care planning (ACP) as a complex health technology in a complex setting such as a nursing home, multiple levels should be targeted, including management, nurses, care staff, volunteers, visiting or residing physicians, families, cleaning or other staff.
Explanation
The implementation process will have a higher chance of succeeding when multiple levels are targeted within the nursing home. Colleagues in the nursing home can help each other to implement the intervention, creating a positive and open environment to learn and develop new skills and deliver the best care possible. In this way the intervention can produce a shift in working culture and attitudes and deliver sustainable change.
Example
The ACP+ intervention targeted not only the (head) nurses, but also other care staff and cleaning, kitchen and maintenance staff. Also, engagement of the management was required for participation in the trial. A few highly motivated people were extensively trained in conducting ACP conversations and this knowledge was past onwards to colleagues via internal training sessions. In this way the whole nursing home was involved in the intervention, leading to greater participation of all nursing home employees.
Read more >
Guidance
Cognitive rehabilitation technology should be accessible physically and in terms of cost, taking into account the mobility problems and the low income of many older people with dementia. To increase the accessibility of technology it is necessary to deliver it at low cost or promote the financing of licenses for people with dementia.
Explanation
Programs for cognitive rehabilitation for people with dementia may be inaccessible due to high costs or difficulty getting access to the location that provides the program because of mobility issues. Technology associated with cognitive rehabilitation or stimulation should be accessible to all those who could benefit from it. Technologies for cognitive rehabilitation should be accessible at home, especially in people living in rural areas or with mobility problems who are not able to travel to a center to perform cognitive rehabilitation.
Read more >
Guidance
The level of cognitive impairment must be taken into account in the design of technology because people with severe dementia have different needs vs. mild dementia.
Explanation and Example
People with severe cognitive impairment will have more problems learning to use different and new devices. They need more explanation and a longer learning time, due to limited cognitive capacities. For example, the clinical experience with Gradior shows that people with moderate and severe dementia should have the therapist as a permanent guide. According to this, Gradior possibly would have to adopt new systems and tools to become effective in people with moderate and severe dementia, and in turn, allow a level of autonomy of the person with dementia who uses this technology. Indeed, the help of a therapist in the first steps of applying a technological-based therapy is strategic for implementing and accepting the approach.
Read more >
Guidance
To improve the implementation of complex health technologies focused on training healthcare professionals in institutional settings, it is important to ensure the involvement of a dedicated trainer throughout the entire implementation process.
Explanation and Examples
For complex health technologies focused on training healthcare professionals, trainers play a crucial role. Trainers should be able to spend dedicated time to deliver the trainings in a specific facility or institution (e.g. nursing home). Hence, they should preferably be paid by a third party or, if paid by the institution, mechanisms should be in place to ensure trainers have dedicated time and training can be delivered.
Ensuring the continuous and long-term involvement of such trainers (e.g. via regional collaborations) could facilitate better implementation of complex health technologies, as timing of the trainings can then be tailored to the needs in a specific context and to the learning needs of the professionals in this context.
Read more >
Guidance
To improve the implementation of complex health technologies in institutional settings, it is important to ensure a clear distinction of roles and responsibilities for staff throughout the entire implementation process.
Explanation and Examples
To facilitate the implementation of complex health technologies in a, often complex, health care setting, a clear distinction of roles and responsibilities for staff is crucial. This clear distinction helps:
- the staff to know what is expected of them,
- co-workers to know what they can ask and expect of the staff involved in the implementation and
- management to determine how much time would be needed for the staff to implement the technology in an appropriate manner.
Read more >
Guidance
To provide high-quality elderly and dementia care, Digital Health Technologies (DHTs) can potentially help achieve the full capacity of Comprehensive Geriatric Assessments (CGAs). In addition they can improve communication and data transfer on patients’ medical and treatment plan information between care settings and stakeholders as well as improve health decision-making. Finally, they can help to share the responsibility of the geriatric assessment between professionals, thereby avoiding overloading the workload of individual users and reducing their psychological stress.
Explanation and Examples:
Due to the higher rate of transitions between care settings in older populations, associated with the complexity of an ageing population and the shift from institutional care to home care, CGAs have become an important assessment tool as they encompass multiple domains and address the variety of complex problems in frail older people. They are considered as multidimensional assessments, using quantitative assessment scales, that support multidisciplinary care teams in clinical decision-making and personalized care planning to meet the needs of older people, their families and carers, focusing on functional status and quality of life.
However, to reach the full potential of CGAs, their implementation should be supported by electronic data systems, which provide relevant outputs and allow timely sharing of information within multidisciplinary teams of healthcare professionals and between different healthcare settings. The use of DHTs can potentially help them reach their full capacity and overcome the data transfer limitations between care settings and stakeholders. To improve the usability and implementation of these DHTs, the following features are recommended: a) accessibility of individual assessment by multiple healthcare professionals and the possibility of splitting sections according to professional expertise to share responsibility for assessments; b) the use of secure data storage, such as clouds; c) automatization of real-time calculation of scales and outcomes with a graphical representation of the person’s profile and health status; d) automatic alerts, notifications and continuous monitoring of item completion; and e) provision of personalized care plans according to the data collected.
Well-designed digital health technologies can contribute to the safety of the potential users (e.g. healthcare professionals and stakeholders) and reduce psychological stress, including burnout and low morale, by avoiding overloading the workload of healthcare professionals. For example, by sharing the responsibility for carrying out the assessments between different professionals.
Read more >
Social Health Domain 1: Fulfill ones potential and obligations
Guidance
To provide informal caregivers of people with dementia living in remote areas with alternative support services, e-learning interventions can overcome some constraints of in-person services, such as costs and transport to the venues, and might increase the reach of services. However, these e-learning interventions should follow a set of recommendations tailored to the rural context in order to be effective.
Explanation and Examples:
E-learning interventions have proven effective in helping caregivers of people living with dementia, with benefits in terms of knowledge about dementia and social and emotional support. The most effective interventions are those with multiple psychotherapeutic components, such as Cognitive Behavioural Therapy and relaxation exercises, educational resources, online peer support groups, and interaction with healthcare professionals.
However, for these interventions to be successful in a specific context, such as that of rural populations, a process of cultural adaptation, co-design and implementation is needed. For example, some of the concerns expressed by the focus groups in our qualitative study into the adaptive implementation of an online support programme for caregivers, iSupport-Spanish version, concerned the local availability of technological devices or internet access in rural areas. Some recommendations that resulted from the process of co-design and cultural adaptation were:
- make the platforms accessible through a personal link instead of a username and password;
- make the platforms available in public spaces for those without access to Wi-Fi or technological devices, e.g. community libraries, town halls, etc.;
- use a multiplatform format (e.g., computer, smartphone, tablets);
- make information available through audio and text (both modalities);
- include images and videos accompanying the text;
- offer the possibility to personalized letter size and background colours;
- avoid technical words (use simple language);
- offer feedback from healthcare professionals and support groups; and
- offer the information in slide format.
Support interventions for caregivers, such as the iSupport-Sp (available at https://learning.bluece.eu/), could improve their quality of life and the quality of care, reduce caregiver burden, improve care service delivery, and could help to cope with care responsibilities.
Read more >
Social Health Domain 2: Manage ones own life and promote independence
Guidance
Researchers and technology developers should be aware of the mutual influence care recipients and caregivers have on each other, and the importance of maintaining and improving caregiving relationships. Therefore they should adopt a dyadic approach to the development, implementation and evaluation of technology-driven interventions by involving both members of the dyad.
Explanation and examples
A mixed-methods feasibility study investigated the impact of a tablet-based activation system on nine community-dwelling caregiving dyads living with dementia, their motivations to use social technology together, and facilitating and impeding factors in the independent use of social technology at home. In light of the SARS-CoV-2 pandemic, it was clear that the extent to which the caregiving dyads were influenced by the extreme social isolation depended on how socially active they were before the pandemic, and their familiarity with social technology. The dyads’ motivations for welcoming technology in their social interactions ranged from trying something new together, keeping up with society to communication support.
Identified facilitators and barriers revealed that user capabilities (care recipients’ cognitive capacities and caregivers’ energy to support their loved ones); user willingness (technology interest) and sufficient support (proactive, continuous and in-person) are three crucial elements in using social technology independently at home.
These contextual factors should be approached from a dyadic perspective taking into account the needs and preferences of both members of the dyad. Technology promoting social participation cannot be developed for people living with dementia without taking into account the needs of their caregivers, and vice versa.
Read more >
Guidance
While designing social assistive robots the following recommended features should be considered to promote successful implementation: low-cost affordable design (pet robot is preferred to humanoid), language mutation for target user and integration with Smart Home IoT (including IoT security mechanisms). During the development phase co-creation should be promoted.
Explanation and Examples:
These recommendations are based on the main findings of a scoping review. The scoping review investigated the state-of-the-art in social assistive robotics, i.e. the current technological advances towards a single framework for effective, safe and secure implementation of social robots for people with dementia. The scoping review qualitatively examined the literature on the use of companion robots, including both pet-like and humanoid robots, and Internet-of-Things (IoT) security, coupled with the new 5G technology for home-based elder care. A comprehensive search strategy was developed and selected databases were looked through with relevant keywords. From the 355 full-text articles found, 90 articles were selected to be examined. In order to ascertain the operation of social assistive robots in the future, remaining challenges, unused opportunities, security risks and suggested remedies are discussed, and a dementia-centred concept and implementation framework proposed.
The following set of recommendations were formulated based on the main findings:
- Consider using a pet robot instead of a humanoid assistive robot as the high cost of the latter for a similar impact and user acceptance cannot be justified.
- Consider low-cost, affordable design and various language mutations for wider deployment in practice, thus allowing more comparative studies, which could provide convincing arguments for using the robot.
- Integrate robot with Smart Home IoT to enhance its functionality towards managing ones own life and promote independence.
- Consider data security, and especially IoT security, prevention mechanisms while integrating the social robot with IoT smart home sensorics.
- Promote wider user involvement and higher level of participation (co-creation) in the development phase of the robot.
- Introduce clearly, and particularly identify, the concerns and needs of people with dementia in the design process.
- List the potential risks and misuses of IoT vulnerabilities, including their remedies, in the design process.
Read more >
Social Health Domain 3: Technology to promote social participation
Guidance
To successfully implement psychosocial applications of technology in dementia care, it is recommended to carry out implementation processes adapted to the context of interest and to adapt training materials socio-culturally.
Explanation/examples:
A qualitative study was performed to trace facilitators and barriers to implementing an evidence-based Dutch psychosocial support programme for people with dementia and carers with greater social integration and better cost-benefit ratio, the Meeting Centres Support Programme (MCSP), in Spanish-speaking countries. Among the potential barriers identified, the most relevant were associated with the lack of adapted training materials to the sociocultural context and the difference between urban and rural populations, particularly the access to populations living in remote areas.
It is therefore recommended that an implementation process be carried out that takes into account the characteristics of the region concerned, in addition to developing actions to overcome specific barriers, such as the creation of technological tools to offer the support programme remotely to provide access to the rural population. For example, as a result of this study, the ‘Introductory Online Course for the Implementation of Meeting Centres for People with Dementia and their Caregivers’ was developed and adapted for Spanish-speaking countries in the Spanish language (available at https://e4you.org/es/moocs/implementacion-de-centros-de-encuentro-para-personas-con-demencia-y-sus-cuidadores). The course consists of eight modules setting out the theoretical background and practical implementation steps in the preparation, implementation and continuation phase.
Also, to offer an alternative to the face-to-face caregivers’ programme included in the MCSP, the iSupport-Sp, an evidence-based training and support programme for caregivers of people with dementia, was developed in an online e-learning format in the Spanish language (available at https://learning.bluece.eu/). This platform aims to offer a support service for caregivers living in remote rural areas in Spain.
Read more >
Guidance
See recommendation no. 3.1.6.7
Read more >








 As the INDUCT project manager, most of my tasks have been ‘behind the scenes’. I have been responsible for submitting scientific deliverables, writing reports for the funder, negotiating deadlines and updating the EU Portal. A project manager functions as a middleman between the EC Project Officer, beneficiaries, partners and ESRs.
As the INDUCT project manager, most of my tasks have been ‘behind the scenes’. I have been responsible for submitting scientific deliverables, writing reports for the funder, negotiating deadlines and updating the EU Portal. A project manager functions as a middleman between the EC Project Officer, beneficiaries, partners and ESRs.